Uterine fibroids are very common non-cancerous (benign) growths that develop in the muscular wall of the uterus. They can range in size from very tiny (a quarter of an inch) to larger than a cantaloupe. Occasionally, they can cause the uterus to grow to the size of a five-month pregnancy. In most cases, there is more than one fibroid in the uterus. While uterine fibroids do not always cause symptoms, their size and location can lead to problems for some women, including pain and heavy bleeding.
Uterine Fibroids can dramatically increase in size during pregnancy. This is thought to occur because of the increase in estrogen levels during pregnancy. After pregnancy, the fibroids usually shrink back to their pre-pregnancy size. They typically improve after menopause when the level of estrogen, the female hormone that circulates in the blood, decreases dramatically. However, menopausal women who are taking supplemental estrogen (hormone replacement therapy) may not experience relief of symptoms.
Uterine fibroids are the most common tumors of the female genital tract. You might hear them referred to as “fibroids” or by several other names, including leiomyoma, leiomyomata, myoma and fibromyoma. Fibroid tumors of the uterus are very common, but for most women, they either do not cause symptoms or cause only minor symptoms.
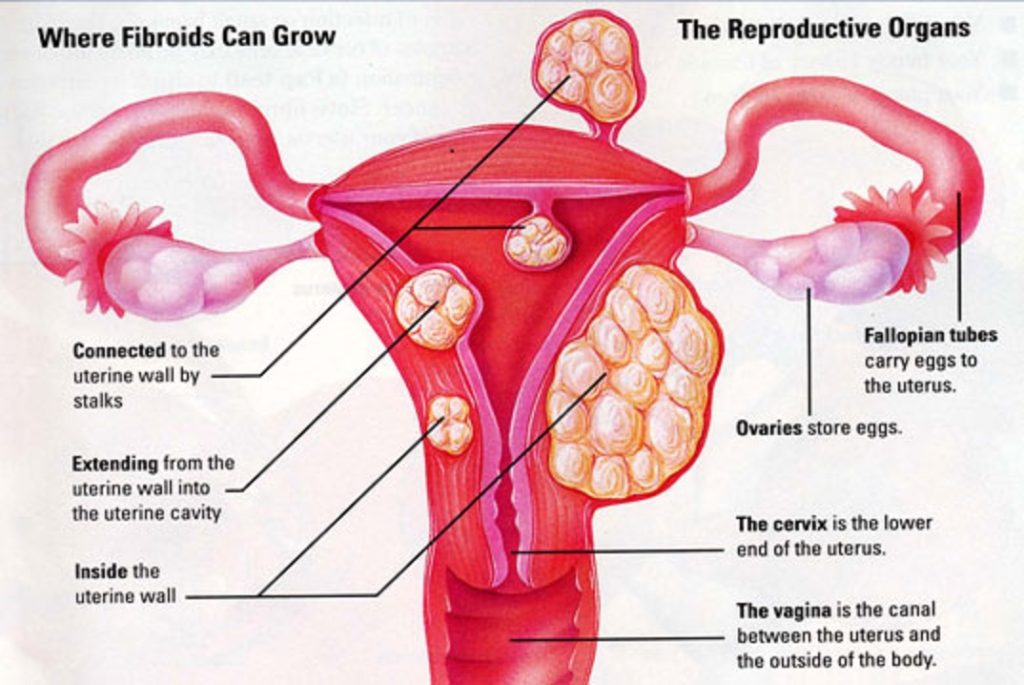
Subserosal Fibroids
These develop under the outside covering of the uterus and expand outward through the wall, giving the uterus a knobby appearance. They typically do not affect a woman’s menstrual flow, but can cause pelvic pain, back pain and generalized pressure. The subserosal fibroid can develop a stalk or stem-like base, making it difficult to distinguish from an ovarian mass. These are called pedunculated. The correct diagnosis can be made with either an ultrasound or magnetic resonance (MR) exam.
Intramural Fibroids
These develop within the lining of the uterus and expand inward, increasing the size of the uterus, and making it feel larger than normal in a gynecologic internal exam. These are the most common fibroids. Intramural fibroids can result in heavier menstrual bleeding and pelvic pain, back pain or the generalized pressure that many women experience.
Submucosal Fibroids
These are just under the lining of the uterus. These are the least common fibroids, but they tend to cause the most problems. Even a very small submucosal fibroid can cause heavy bleeding – gushing, very heavy and prolonged periods.
Prevalence of Uterine Fibroids
Twenty to 40 percent of women age 35 and older have uterine fibroids of a significant size. African American women are at a higher risk for fibroids: as many as 50 percent have fibroids of a significant size. Uterine fibroids are the most frequent indication for hysterectomy in premenopausal women and, therefore, are a major public health issue. Of the 600,000 hysterectomies performed annually in the United States, one-third are due to fibroids
Uterine Fibroid Symptoms
Most uterine fibroids don’t cause symptoms—only 10 to 20 percent of women who have fibroids require treatment. Depending on size, location and number of fibroids, they may cause:
- Heavy, prolonged menstrual periods and unusual monthly bleeding, sometimes with clots; this can lead to anemia
- Pelvic pain and pressure
- Pain in the back and legs
- Pain during sexual intercourse
- Bladder pressure leading to a frequent urge to urinate
- Pressure on the bowel, leading to constipation and bloating
- Abnormally enlarged abdomen
Imaging Expertise Enables Interventional Radiologists to Provide Gynecologists and Their Patients Better Diagnosis and Nonsurgical Treatment Options
Women typically undergo an ultrasound at their gynecologist’s office as part of the evaluation process to https://functionalmedcenter.com/ determine the presence of uterine fibroids. It is a rudimentary imaging tool for fibroids that often does not show other underlying diseases or all the existing fibroids. For this reason, MRI is the standard imaging tool used by interventional radiologists.
Magnetic resonance imaging (MRI) improves the patient selection for who should receive nonsurgical uterine fibroid embolization (UFE) to kill their tumors. Interventional radiologists can use MRIs to determine if a tumor can be embolized, detect alternate causes for the symptoms, identify pathology that could prevent a women from having UFE and avoid ineffective treatments. Using an MRI rather than ultrasound is like listening to a digital CD rather than a record – the quality is better in every way. By working with a patient’s gynecologist, interventional radiologists can use MRIs to enhance the level of patient care through better diagnosis, better education, better treatment options and better outcomes.
Second Opinion Prior to Hysterectomy
For true informed consent before surgery, patients should be aware of all of their treatment options. Patients considering surgical treatment should also get a second opinion from Dr Jerry, who is most qualified to interpret the MRI and determine if they are candidates for the interventional procedure.
- Call to schedule a consultation: During your consultation you will be able to ask questions and be answered by a medical professional. This step will help you make an informed decision on whether embolization or hysterectomy is the right choice for you. Call 727-386-9981
- Day of consultation: Please arrive 20 minutes before your appointment to fill out necessary paperwork and a health questionnaire. Bring any patient history such as (pap smear results, ultrasound or MRI imaging and notes from your primary care doctor or gynecologist). During your consultation you will be able to ask questions plus get knowledgeable information to help you make an informed and educated decision on what procedure works best for you on treating your fibroids.
- Return for MRI: Once you have decided to continue with the fibroid embolization, you will be scheduled for an MRI if you have not already had one. An MRI will provide us with images to prepare for your procedure.
- The day of your procedure: Please arrive 20 minutes before your appointment time to fill out additional paperwork and to go over simple instructions for your return home. Fibroid Embolization is a same day procedure, so you will be returning home that day with only a few days of down time. Please be sure to have someone with you. This person will be given a prescription for pain management as you will have minimal cramping and discomfort for a few days.
